

| << Chapter < Page | Chapter >> Page > |
Viruses that infect plants are considered biotrophic parasites, which means that they can establish an infection without killing the host, similar to what is observed in the lysogenic life cycles of bacteriophages. Viral infection can be asymptomatic (latent) or can lead to cell death (lytic infection). The life cycle begins with the penetration of the virus into the host cell. Next, the virus is uncoated within the cytoplasm of the cell when the capsid is removed. Depending on the type of nucleic acid, cellular components are used to replicate the viral genome and synthesize viral proteins for assembly of new virions. To establish a systemic infection, the virus must enter a part of the vascular system of the plant, such as the phloem. The time required for systemic infection may vary from a few days to a few weeks depending on the virus, the plant species, and the environmental conditions. The virus life cycle is complete when it is transmitted from an infected plant to a healthy plant.
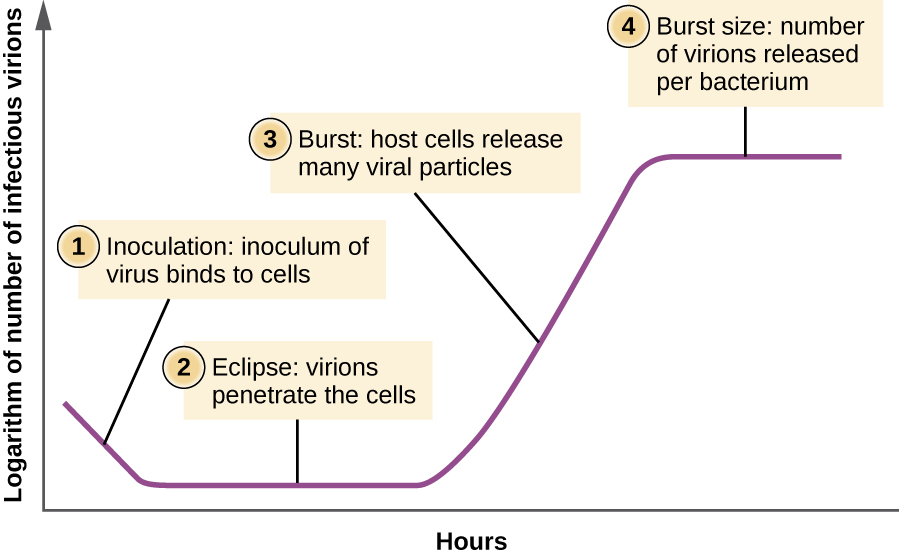
Unlike the growth curve for a bacterial population, the growth curve for a virus population over its life cycle does not follow a sigmoidal curve. During the initial stage, an inoculum of virus causes infection. In the eclipse phase , viruses bind and penetrate the cells with no virions detected in the medium. The chief difference that next appears in the viral growth curve compared to a bacterial growth curve occurs when virions are released from the lysed host cell at the same time. Such an occurrence is called a burst , and the number of virions per bacterium released is described as the burst size . In a one-step multiplication curve for bacteriophage , the host cells lyse, releasing many viral particles to the medium, which leads to a very steep rise in viral titer (the number of virions per unit volume). If no viable host cells remain, the viral particles begin to degrade during the decline of the culture (see [link] ).
Ebola is incurable and deadly. The outbreak in West Africa in 2014 was unprecedented, dwarfing other human Ebola epidemics in the level of mortality. Of 24,666 suspected or confirmed cases reported, 10,179 people died. World Health Organization. “WHO Ebola Data and Statistics.” March 18, 2005. http://apps.who.int/gho/data/view.ebola-sitrep.ebola-summary-20150318?lang=en
No approved treatments or vaccines for Ebola are available. While some drugs have shown potential in laboratory studies and animal models, they have not been tested in humans for safety and effectiveness. Not only are these drugs untested or unregistered but they are also in short supply.
Given the great suffering and high mortality rates, it is fair to ask whether unregistered and untested medications are better than none at all. Should such drugs be dispensed and, if so, who should receive them, in light of their extremely limited supplies? Is it ethical to treat untested drugs on patients with Ebola? On the other hand, is it ethical to withhold potentially life-saving drugs from dying patients? Or should the drugs perhaps be reserved for health-care providers working to contain the disease?
In August 2014, two infected US aid workers and a Spanish priest were treated with ZMapp , an unregistered drug that had been tested in monkeys but not in humans. The two American aid workers recovered, but the priest died. Later that month, the WHO released a report on the ethics of treating patients with the drug. Since Ebola is often fatal, the panel reasoned that it is ethical to give the unregistered drugs and unethical to withhold them for safety concerns. This situation is an example of “compassionate use” outside the well-established system of regulation and governance of therapies.
On September 24, 2014, Thomas Eric Duncan arrived at the Texas Health Presbyterian Hospital in Dallas complaining of a fever, headache, vomiting, and diarrhea—symptoms commonly observed in patients with the cold or the flu. After examination, an emergency department doctor diagnosed him with sinusitis, prescribed some antibiotics, and sent him home. Two days later, Duncan returned to the hospital by ambulance. His condition had deteriorated and additional blood tests confirmed that he has been infected with the Ebola virus.
Further investigations revealed that Duncan had just returned from Liberia, one of the countries in the midst of a severe Ebola epidemic. On September 15, nine days before he showed up at the hospital in Dallas, Duncan had helped transport an Ebola-stricken neighbor to a hospital in Liberia. The hospital continued to treat Duncan, but he died several days after being admitted.
The timeline of the Duncan case is indicative of the life cycle of the Ebola virus. The incubation time for Ebola ranges from 2 days to 21 days. Nine days passed between Duncan’s exposure to the virus infection and the appearance of his symptoms. This corresponds, in part, to the eclipse period in the growth of the virus population. During the eclipse phase, Duncan would have been unable to transmit the disease to others. However, once an infected individual begins exhibiting symptoms, the disease becomes very contagious. Ebola virus is transmitted through direct contact with droplets of bodily fluids such as saliva, blood, and vomit. Duncan could conceivably have transmitted the disease to others at any time after he began having symptoms, presumably some time before his arrival at the hospital in Dallas. Once a hospital realizes a patient like Duncan is infected with Ebola virus, the patient is immediately quarantined, and public health officials initiate a back trace to identify everyone with whom a patient like Duncan might have interacted during the period in which he was showing symptoms.
Public health officials were able to track down 10 high-risk individuals (family members of Duncan) and 50 low-risk individuals to monitor them for signs of infection. None contracted the disease. However, one of the nurses charged with Duncan’s care did become infected. This, along with Duncan’s initial misdiagnosis, made it clear that US hospitals needed to provide additional training to medical personnel to prevent a possible Ebola outbreak in the US.


For additional information about Ebola, please visit the CDC website.
An enzyme from HIV that can make a copy of DNA from RNA is called _______________________.
reverse transcriptase
For lytic viruses, _________________ is a phase during a viral growth curve when the virus is not detected.
eclipse
Briefly explain the difference between the mechanism of entry of a T-even bacteriophage and an animal virus.
Discuss the difference between generalized and specialized transduction.
Differentiate between lytic and lysogenic cycles.
Notification Switch
Would you like to follow the 'Microbiology' conversation and receive update notifications?

|
|
|
|
|

|
|

|
|

|
|

|
|
|
|
|

|
|

|
|

|