

| << Chapter < Page | Chapter >> Page > |
For the optimum treatment of some infections, two antibacterial drugs may be administered together to provide a synergistic interaction that is better than the efficacy of either drug alone. A classic example of synergistic combinations is trimethoprim and sulfamethoxazole ( Bactrim ). Individually, these two drugs provide only bacteriostatic inhibition of bacterial growth, but combined, the drugs are bactericidal .
Whereas synergistic drug interactions provide a benefit to the patient, antagonistic interactions produce harmful effects. Antagonism can occur between two antimicrobials or between antimicrobials and nonantimicrobials being used to treat other conditions. The effects vary depending on the drugs involved, but antagonistic interactions may cause loss of drug activity, decreased therapeutic levels due to increased metabolism and elimination, or increased potential for toxicity due to decreased metabolism and elimination. As an example, some antibacterials are absorbed most effectively from the acidic environment of the stomach. If a patient takes antacids, however, this increases the pH of the stomach and negatively impacts the absorption of these antimicrobials, decreasing their effectiveness in treating an infection. Studies have also shown an association between use of some antimicrobials and failure of oral contraceptives. B.D. Dickinson et al. “Drug Interactions between Oral Contraceptives and Antibiotics.” Obstetrics&Gynecology 98, no. 5 (2001):853–860.
In the United States and many other countries, most antimicrobial drugs are self-administered by patients at home. Unfortunately, many patients stop taking antimicrobials once their symptoms dissipate and they feel better. If a 10-day course of treatment is prescribed, many patients only take the drug for 5 or 6 days, unaware of the negative consequences of not completing the full course of treatment. A shorter course of treatment not only fails to kill the target organisms to expected levels, it also selects for drug-resistant variants within the target population and within the patient’s microbiota.
Patients’ nonadherence especially amplifies drug resistance when the recommended course of treatment is long. Treatment for tuberculosis (TB) is a case in point, with the recommended treatment lasting from 6 months to a year. The CDC estimates that about one-third of the world’s population is infected with TB, most living in underdeveloped or underserved regions where antimicrobial drugs are available over the counter. In such countries, there may be even lower rates of adherence than in developed areas. Nonadherence leads to antibiotic resistance and more difficulty in controlling pathogens. As a direct result, the emergence of multidrug-resistant and extensively drug-resistant strains of TB is becoming a huge problem.
Overprescription of antimicrobials also contributes to antibiotic resistance. Patients often demand antibiotics for diseases that do not require them, like viral colds and ear infections. Pharmaceutical companies aggressively market drugs to physicians and clinics, making it easy for them to give free samples to patients, and some pharmacies even offer certain antibiotics free to low-income patients with a prescription.
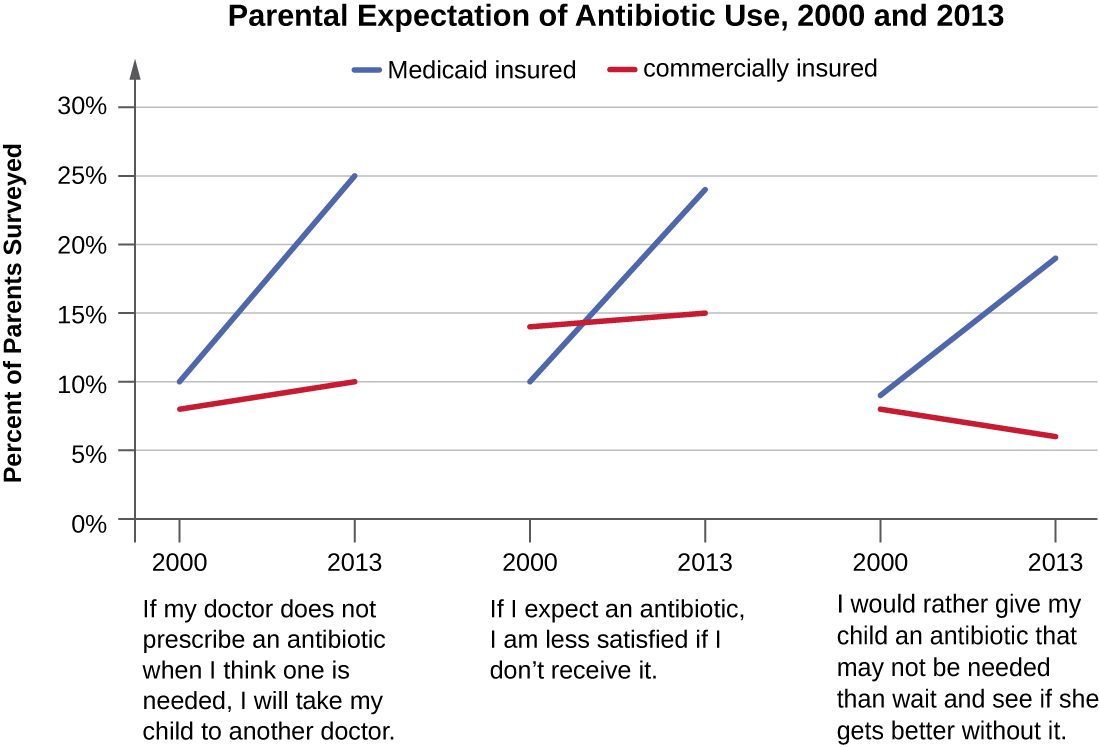
In recent years, various initiatives have aimed to educate parents and clinicians about the judicious use of antibiotics. However, a recent study showed that, between 2000 and 2013, the parental expectation for antimicrobial prescriptions for children actually increased ( [link] ).
One possible solution is a regimen called directly observed therapy (DOT) , which involves the supervised administration of medications to patients. Patients are either required to visit a health-care facility to receive their medications, or health-care providers must administer medication in patients’ homes or another designated location. DOT has been implemented in many cases for the treatment of TB and has been shown to be effective; indeed, DOT is an integral part of WHO’s global strategy for eradicating TB. Centers for Disease Control and Prevention. “Tuberculosis (TB).” http://www.cdc.gov/tb/education/ssmodules/module9/ss9reading2.htm. Accessed June 2, 2016. , World Health Organization. “Tuberculosis (TB): The Five Elements of DOTS.” http://www.who.int/tb/dots/whatisdots/en/. Accessed June 2, 2016. But is this a practical strategy for all antibiotics? Would patients taking penicillin, for example, be more or less likely to adhere to the full course of treatment if they had to travel to a health-care facility for each dose? And who would pay for the increased cost associated with DOT? When it comes to overprescription, should someone be policing physicians or drug companies to enforce best practices? What group should assume this responsibility, and what penalties would be effective in discouraging overprescription?
The bacterium known for causing pseudomembranous colitis, a potentially deadly superinfection, is ________.
Clostridium difficile
Narrow-spectrum antimicrobials are commonly used for prophylaxis following surgery.
False
When prescribing antibiotics, what aspects of the patient’s health history should the clinician ask about and why?
When is using a broad-spectrum antimicrobial drug warranted?
Notification Switch
Would you like to follow the 'Microbiology' conversation and receive update notifications?

|
|

|
|

|
|

|
|

|
|

|
|

|
|

|
|

|
|

|