

| << Chapter < Page | Chapter >> Page > |
The distal end of the femur has medial and lateral bony expansions. On the lateral side, the smooth portion that covers the distal and posterior aspects of the lateral expansion is the lateral condyle of the femur . The roughened area on the outer, lateral side of the condyle is the lateral epicondyle of the femur . Similarly, the smooth region of the distal and posterior medial femur is the medial condyle of the femur , and the irregular outer, medial side of this is the medial epicondyle of the femur . The lateral and medial condyles articulate with the tibia to form the knee joint. The epicondyles provide attachment for muscles and supporting ligaments of the knee. The adductor tubercle is a small bump located at the superior margin of the medial epicondyle. Posteriorly, the medial and lateral condyles are separated by a deep depression called the intercondylar fossa . Anteriorly, the smooth surfaces of the condyles join together to form a wide groove called the patellar surface , which provides for articulation with the patella bone. The combination of the medial and lateral condyles with the patellar surface gives the distal end of the femur a horseshoe (U) shape.
Watch this video to view how a fracture of the mid-femur is surgically repaired. How are the two portions of the broken femur stabilized during surgical repair of a fractured femur?
The patella (kneecap) is largest sesamoid bone of the body (see [link] ). A sesamoid bone is a bone that is incorporated into the tendon of a muscle where that tendon crosses a joint. The sesamoid bone articulates with the underlying bones to prevent damage to the muscle tendon due to rubbing against the bones during movements of the joint. The patella is found in the tendon of the quadriceps femoris muscle, the large muscle of the anterior thigh that passes across the anterior knee to attach to the tibia. The patella articulates with the patellar surface of the femur and thus prevents rubbing of the muscle tendon against the distal femur. The patella also lifts the tendon away from the knee joint, which increases the leverage power of the quadriceps femoris muscle as it acts across the knee. The patella does not articulate with the tibia.
Visit this site to perform a virtual knee replacement surgery. The prosthetic knee components must be properly aligned to function properly. How is this alignment ensured?
Patellofemoral syndrome may be initiated by a variety of causes, including individual variations in the shape and movement of the patella, a direct blow to the patella, or flat feet or improper shoes that cause excessive turning in or out of the feet or leg. These factors may cause in an imbalance in the muscle pull that acts on the patella, resulting in an abnormal tracking of the patella that allows it to deviate too far toward the lateral side of the patellar surface on the distal femur.
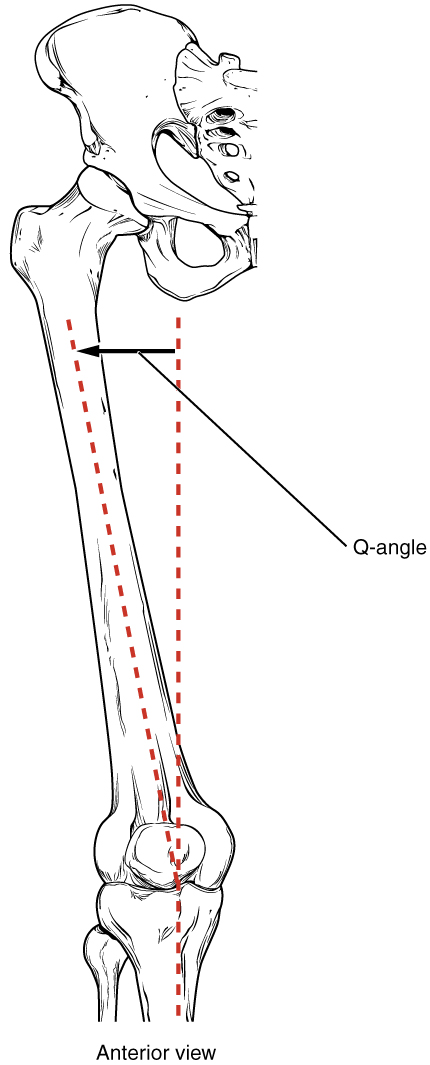
Because the hips are wider than the knee region, the femur has a diagonal orientation within the thigh, in contrast to the vertically oriented tibia of the leg ( [link] ). The Q-angle is a measure of how far the femur is angled laterally away from vertical. The Q-angle is normally 10–15 degrees, with females typically having a larger Q-angle due to their wider pelvis. During extension of the knee, the quadriceps femoris muscle pulls the patella both superiorly and laterally, with the lateral pull greater in women due to their large Q-angle. This makes women more vulnerable to developing patellofemoral syndrome than men. Normally, the large lip on the lateral side of the patellar surface of the femur compensates for the lateral pull on the patella, and thus helps to maintain its proper tracking.
However, if the pull produced by the medial and lateral sides of the quadriceps femoris muscle is not properly balanced, abnormal tracking of the patella toward the lateral side may occur. With continued use, this produces pain and could result in damage to the articulating surfaces of the patella and femur, and the possible future development of arthritis. Treatment generally involves stopping the activity that produces knee pain for a period of time, followed by a gradual resumption of activity. Proper strengthening of the quadriceps femoris muscle to correct for imbalances is also important to help prevent reoccurrence.
Notification Switch
Would you like to follow the 'Anatomy & Physiology: support and movement' conversation and receive update notifications?

|
|

|
|

|
|

|
|
|
|
|
|
|
|
|
|

|
|

|
|

|