

| << Chapter < Page | Chapter >> Page > |
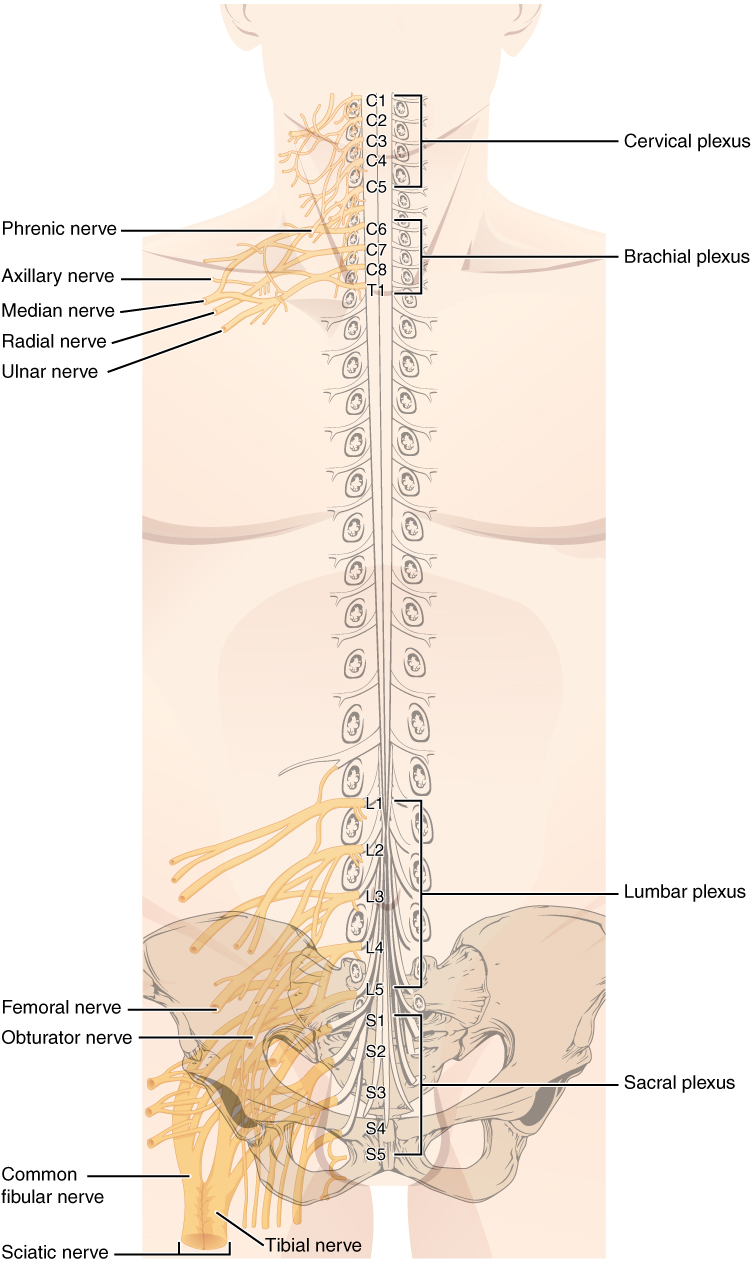
These plexuses are described as arising from spinal nerves and giving rise to certain systemic nerves, but they contain fibers that serve sensory functions or fibers that serve motor functions. This means that some fibers extend from cutaneous or other peripheral sensory surfaces and send action potentials into the CNS. Those are axons of sensory neurons in the dorsal root ganglia that enter the spinal cord through the dorsal nerve root. Other fibers are the axons of motor neurons of the anterior horn of the spinal cord, which emerge in the ventral nerve root and send action potentials to cause skeletal muscles to contract in their target regions. For example, the radial nerve contains fibers of cutaneous sensation in the arm, as well as motor fibers that move muscles in the arm.
Spinal nerves of the thoracic region, T2 through T11, are not part of the plexuses but rather emerge and give rise to the intercostal nerves found between the ribs, which articulate with the vertebrae surrounding the spinal nerve.
Smell is an important sense, especially for the enjoyment of food. There are only five tastes sensed by the tongue, and two of them are generally thought of as unpleasant tastes (sour and bitter). The rich sensory experience of food is the result of odor molecules associated with the food, both as food is moved into the mouth, and therefore passes under the nose, and when it is chewed and molecules are released to move up the pharynx into the posterior nasal cavity. Anosmia results in a loss of the enjoyment of food.
As the replacement of olfactory neurons declines with age, anosmia can set in. Without the sense of smell, many sufferers complain of food tasting bland. Often, the only way to enjoy food is to add seasoning that can be sensed on the tongue, which usually means adding table salt. The problem with this solution, however, is that this increases sodium intake, which can lead to cardiovascular problems through water retention and the associated increase in blood pressure.
The PNS is composed of the groups of neurons (ganglia) and bundles of axons (nerves) that are outside of the brain and spinal cord. Ganglia are of two types, sensory or autonomic. Sensory ganglia contain unipolar sensory neurons and are found on the dorsal root of all spinal nerves as well as associated with many of the cranial nerves. Autonomic ganglia are in the sympathetic chain, the associated paravertebral or prevertebral ganglia, or in terminal ganglia near or within the organs controlled by the autonomic nervous system.
Nerves are classified as cranial nerves or spinal nerves on the basis of their connection to the brain or spinal cord, respectively. The twelve cranial nerves can be strictly sensory in function, strictly motor in function, or a combination of the two functions. Sensory fibers are axons of sensory ganglia that carry sensory information into the brain and target sensory nuclei. Motor fibers are axons of motor neurons in motor nuclei of the brain stem and target skeletal muscles of the head and neck. Spinal nerves are all mixed nerves with both sensory and motor fibers. Spinal nerves emerge from the spinal cord and reorganize through plexuses, which then give rise to systemic nerves. Thoracic spinal nerves are not part of any plexus, but give rise to the intercostal nerves directly.
[link] If you zoom in on the DRG, you can see smaller satellite glial cells surrounding the large cell bodies of the sensory neurons. From what structure do satellite cells derive during embryologic development?
[link] They derive from the neural crest.
[link] To what structures in a skeletal muscle are the endoneurium, perineurium, and epineurium comparable?
[link] The endoneurium surrounding individual nerve fibers is comparable to the endomysium surrounding myofibrils, the perineurium bundling axons into fascicles is comparable to the perimysium bundling muscle fibers into fascicles, and the epineurium surrounding the whole nerve is comparable to the epimysium surrounding the muscle.
Visit this site to read about a man who wakes with a headache and a loss of vision. His regular doctor sent him to an ophthalmologist to address the vision loss. The ophthalmologist recognizes a greater problem and immediately sends him to the emergency room. Once there, the patient undergoes a large battery of tests, but a definite cause cannot be found. A specialist recognizes the problem as meningitis, but the question is what caused it originally. How can that be cured? The loss of vision comes from swelling around the optic nerve, which probably presented as a bulge on the inside of the eye. Why is swelling related to meningitis going to push on the optic nerve?
The optic nerve enters the CNS in its projection from the eyes in the periphery, which means that it crosses through the meninges. Meningitis will include swelling of those protective layers of the CNS, resulting in pressure on the optic nerve, which can compromise vision.
Notification Switch
Would you like to follow the 'Anatomy & Physiology' conversation and receive update notifications?

|
|
|
|
|

|
|

|
|

|
|
|
|
|

|
|

|
|

|
|

|
|

|
|
|
|